Club Foot

What is Club foot?
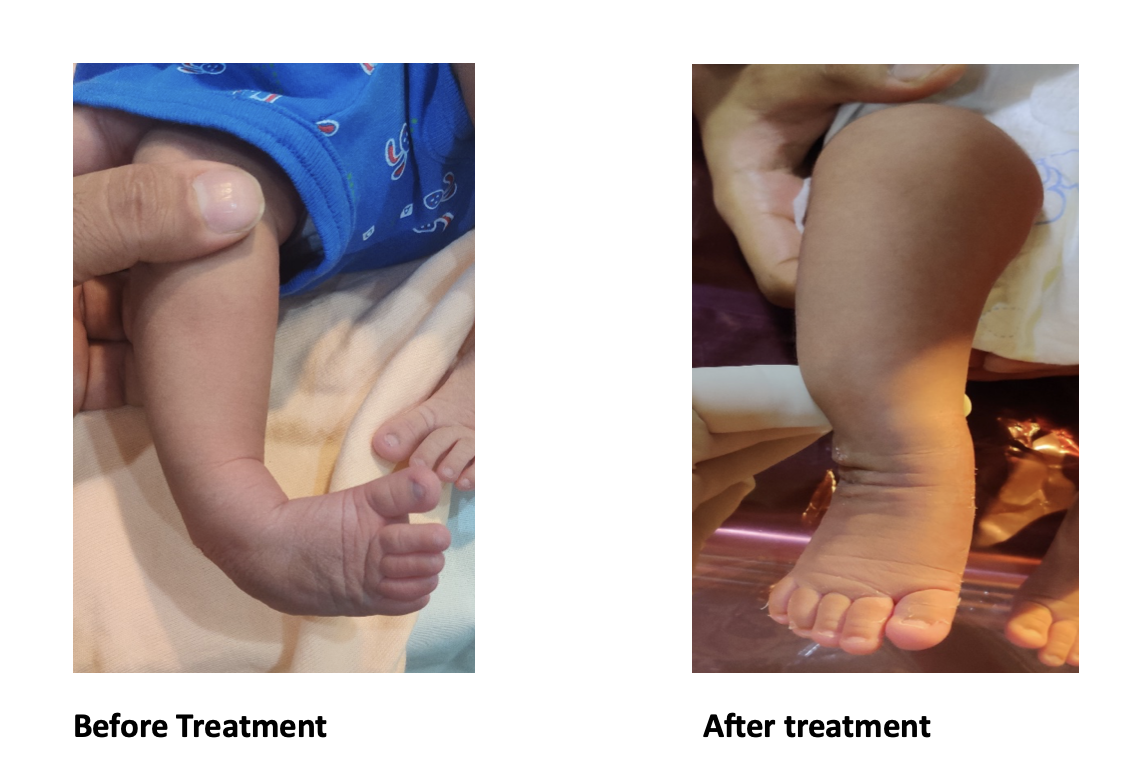
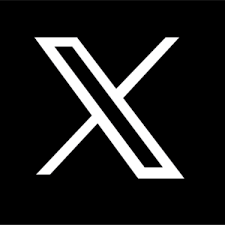
Club foot is a deformity of feet in infants in which the foot is rotated inwards and downwards with the heel facing upwards and in. The affected foot may also be slightly shorter and thinner than the other. 1 in a 1000 babies are usually affected with males being more affected. It is usually diagnosed at birth but can be detected in a prenatal ultrasound.
What are the causes of club foot?
A: Both Genetic and environmental factors may play a role. There is increased risk in families with a history of club feet.
What are the types of club foot?
A Club foot is classified into 2 types:
1- Idiopathic or isolated
2- Syndromic club foot associated with neuromuscular conditions like spina bifida, arthrogryposis, Ehler’s Danlos Syndrome, etc. These types are more resistant to treatment, requiring longer nonsurgical or surgical treatment.
What is the treatment of club foot?
A Club foot without treatment will not resolve on its own. Initially the foot is not painful in spite of the deformity, but if left untreated the child will walk on the outer sider of the foot, develop callosities , will be unable to wear shoes and will develop a lifelong painful gait.
1- Casting: The PONSETI method is the most common method of club foot treatment. It involves gentle stretching and plastering the lower limb from toe to groin in successive corrective casts. The casts are usually changed weekly until the deformity is completely corrected usually by the end of 6-8 weeks.
2- Achilles Tenotomy:

At the end of the corrective casts, the doctor will need to cut the contracted heel cord with a small incision at the back of the heel and give a final plater for 3 weeks. This allows the heel cord to heal in an elongated position.
3- Bracing:

After the correction is achieved, the foot has a natural tendency to revert back to the deformed position. This is prevented by putting the feet in a brace for a few years. The club foot brace has a curved steel bar attached between the 2 feet and lace up shoes which hold the feet in an outward rotated position. This needs to be worn for at least 23 hrs for the first 3 months and then at night and nap time for 14-16 hrs a day until the child is 5 yrs of age. The child may be fussy about the brace initially but will gradually get accustomed to wearing it.
Surgery:
Most club feet can be successfully treated with casting and bracing. However, some resistant cases may need surgery for correction of the deformity. This may involve releasing or lengthening the tight structures around the foot or transferring some tendons to balance the muscle forces around the foot. Some stiff feet may also require cutting of bones to realign them.
Conclusion:
All club feet require treatment. They do not get better on their own. Nonsurgical Ponseti method of treatment is usually successful in treating most club feet with no residual deformity. A small percentage of club feet require surgical treatment for deformity correction.